
🎧 Can AI Stop GLP-1 Patients From Churning? Ep.8 with Dr. Paul Sacher
How DTC platforms are keeping customers without lowering prices

Watch on Youtube
Listen on Spotify
Read the transcript with ChatGPT
Preventing churn in the UK GLP-1 market is like trying to grab a fistful of water. The drug has commoditized, which means patients see providers as interchangeable distributors of the same product. Once that happens, price is the only differentiator. If the customer believes that five companies are selling the same pen, why wouldn’t they choose the cheapest one?
This behavior tanks the lifetime value of customers, because it encourages switching. While this dynamic could be easier to stomach if the market were growing fast enough to replace churned customers, the market has been stagnant for the past several months.
So, instead of competing for fresh demand, providers are fighting over the same pool of existing customers, which leads to price-undercutting via discounts. Providers now face the miserable situation of shrinking margins, which will continue to shrink as long as customers keep punting their provider in favor of a cheaper alternative.
Then the question is: Can providers differentiate themselves with something other than price? And can AI-enabled platforms give patients a reason to stay long enough to turn a profit?
I sat down with Dr. Paul Sacher to understand what AI can do as of this moment. Paul has spent more than two decades in obesity management and has worked across digital-health providers building and evaluating patient-facing AI systems. His team has analysed close to 100,000 support tickets, churn data, and patient interviews, which makes this a practical conversation rather than another abstract debate about healthcare chatbots.
If there is anyone who understands both the promise and the failure-modes of AI in GLP-1 care, it’s Paul.
Here are my three key takeaways.
Sponsorships are now fully booked through the end of 2026. If you’d like to discuss a Q1 2027 partnership with GLP-1 Digest, get in touch.
1. Predict the customer’s next sticking-point
Whether someone is going to re-order with you depends on how accurately you can predict and respond to that customer’s sticking-points. Sticking points are high-risk events that lead to churn, and can be categorized based on where the patient is on their weight-loss journey.
For example, side-effects: this is the first sticking-point people experience, usually within the first four weeks of a new GLP-1 treatment. No one wants to be sitting on the toilet at work, feeling sick, and receive a notification from their GLP-1 app about eating healthy food.
The other main sticking-point is when people experience a weight-loss plateau. Patients get concerned or complain, which leads to a noticeable increase in cost to serve. In this case, the treatment hasn’t met the customer’s expectations and they are of two minds about carrying on.
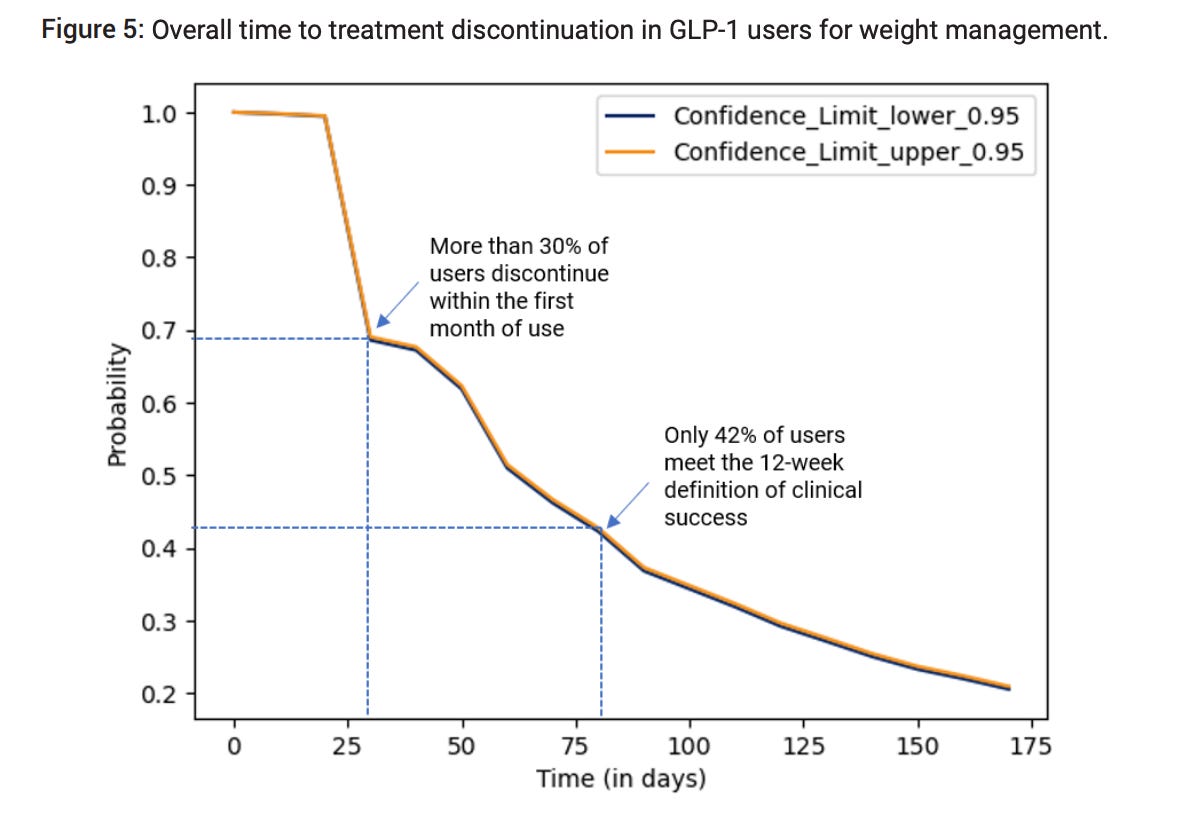
DTC platforms can predict these sticking-points with high accuracy, but many do nothing about it. If you let a customer reach these points without any intervention or support, you deserve to lose that customer to a competitor. It’s frankly lazy to let customers be blindsided by side effects or weight-loss plateaus when these platforms are sitting on millions of data points—weight-loss trajectories, side effect reports, refill behaviour, baseline BMI, dose history, comorbidities, and patient messages—that could predict such challenges.
You should be able to build an accurate clinical performance model using frontier AI models to determine what a patient’s journey will plausibly look like, and regularly check whether they have deviated from the expectation.
Any deviation from the model should trigger proactive messaging to prevent the patient from churning. It might simply be a message before an expected plateau, or faster side-effect support after titration, or introducing maintenance plans as the patient approaches goal-weight.
This is what personalization looks like in a highly scalable and efficient manner, and this is what will keep a patient on board even when there is a cheaper pen available from some other care-platform.
2. AI can create operating leverage without removing the human coach
In a market with shrinking margins and price-competition, you can’t scale by just hiring more clinicians to field a higher volume of patient interactions.
Paul explained that many patient queries do not need a clinician or coach in the first place, especially questions about side effects and nutrition. An AI chatbot can fairly accurately respond to a patient who is asking whether nausea is normal, how to manage constipation, what to eat when appetite disappears, or how much protein they need per day.
These types of queries just need an immediate, reassuring answer and can absorb much of the low-touch, high-volume support tickets that would otherwise fill the medical team’s inbox. Implementing an AI chatbot would free up clinicians and health coaches for escalated tickets, to spend their time working on actual behavior-change, where human judgment is essential (for now).
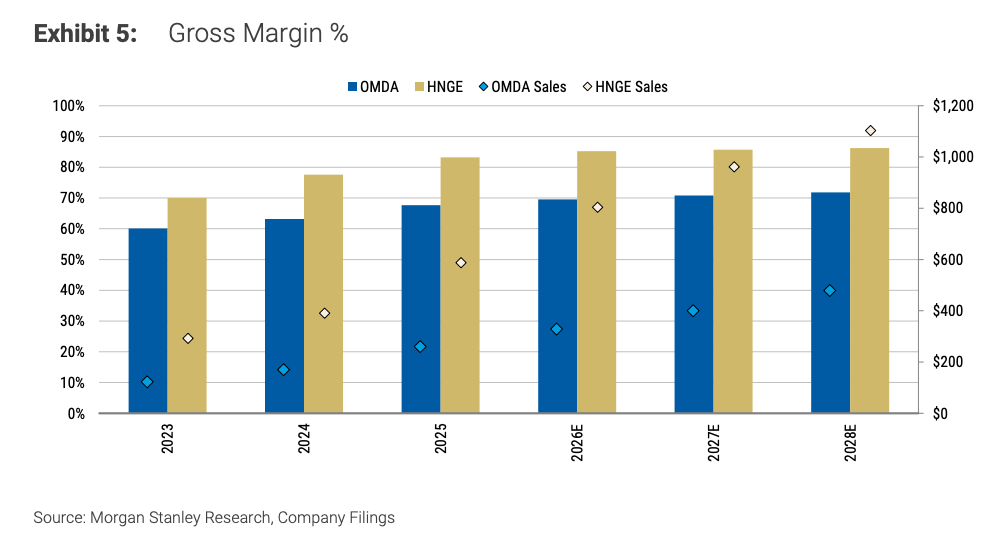
One provider that looks closest to this model is Omada Health with OmadaSpark, its member-facing AI assistant inside its broader Nutrition Intelligence feature. Omada is using AI to absorb high-volume, lower-acuity nutrition and lifestyle questions, give members immediate support, and then pass useful context back to human care teams for escalation or deeper behavior-change work.
Morgan Stanley notes that Omada’s broader technology and AI tools have helped drive a roughly 25% increase in members per coach and contributed to gross margin expanding by about 11% over two years. Omada scaled up and improved margins without hiring any new clinicians.
3. How do you retain patients once they’ve reached their goal weight?
Many DTC providers have spent the last two years trying to get as many patients onto GLP-1s as possible, and with that, have squeezed as much juice as they can from the onboarding experience. But some patients are now reaching eight months of treatment or beyond, and there is still very little support around weight-maintenance or what that means from a broader health perspective.
How do you incentivize patients to keep paying for treatment once they’ve reached their goal-weight?
This requires a complete revamp in product messaging that centers around the extraordinary health gains to be had by continuing to take the drug, such as lower blood pressure, lower cholesterol, and gains in quality of life metrics that make people feel great.
But, admittedly, if you manage to achieve this level of patient education, then bravo, because most customers never receive (or retain) the nuanced clinical picture required to see obesity as a chronic disease.
The second question is how do you make maintenance-customers economically valuable when they are no longer ordering every month?
A lower-cost maintenance model converts what would otherwise be lost customers into higher-lifetime-value relationships, which is far better than simply losing them forever. At the same time, it resolves the final sticking point in the customers journey by giving them a clear, affordable path to sustain the health gains they’ve already achieved.
**The views, opinions, and recommendations expressed in this essay are solely my own and do not represent the views, policies, or positions of any other organization with which I am affiliated. This content is provided for informational purposes only and should not be considered medical, legal or investment advice.**