
What Do GLP-1 Patients Actually Want?
Losing weight is just the beginning


Hello and happy Sunday! Was this newsletter forwarded to you? Sign up to get it in your inbox.
I spent most of this week camped out in my home office, a cozy sanctuary overflowing with plants that’s now starting to resemble a tiny jungle. I don’t mind. Between chewing pens like it's finals week (embarrassingly difficult habit to kill) and fighting off waves of dread for sitting in one place for too long, I had one question this week:
Once GLP-1 patients drop the weight, what exactly do they want next?
Yes, we've covered the obvious ground. They feel healthier, might shop differently, and may even find themselves logging hours in a new hobby. But surely something deeper is happening here, right? Something interesting hiding just out of sight that the headlines haven’t figured out yet.
That's exactly the sort of rabbit hole I want to explore.
Welcome back to the GLP-1 Digest.
Let's dig in.
📊 Inside the Numbers
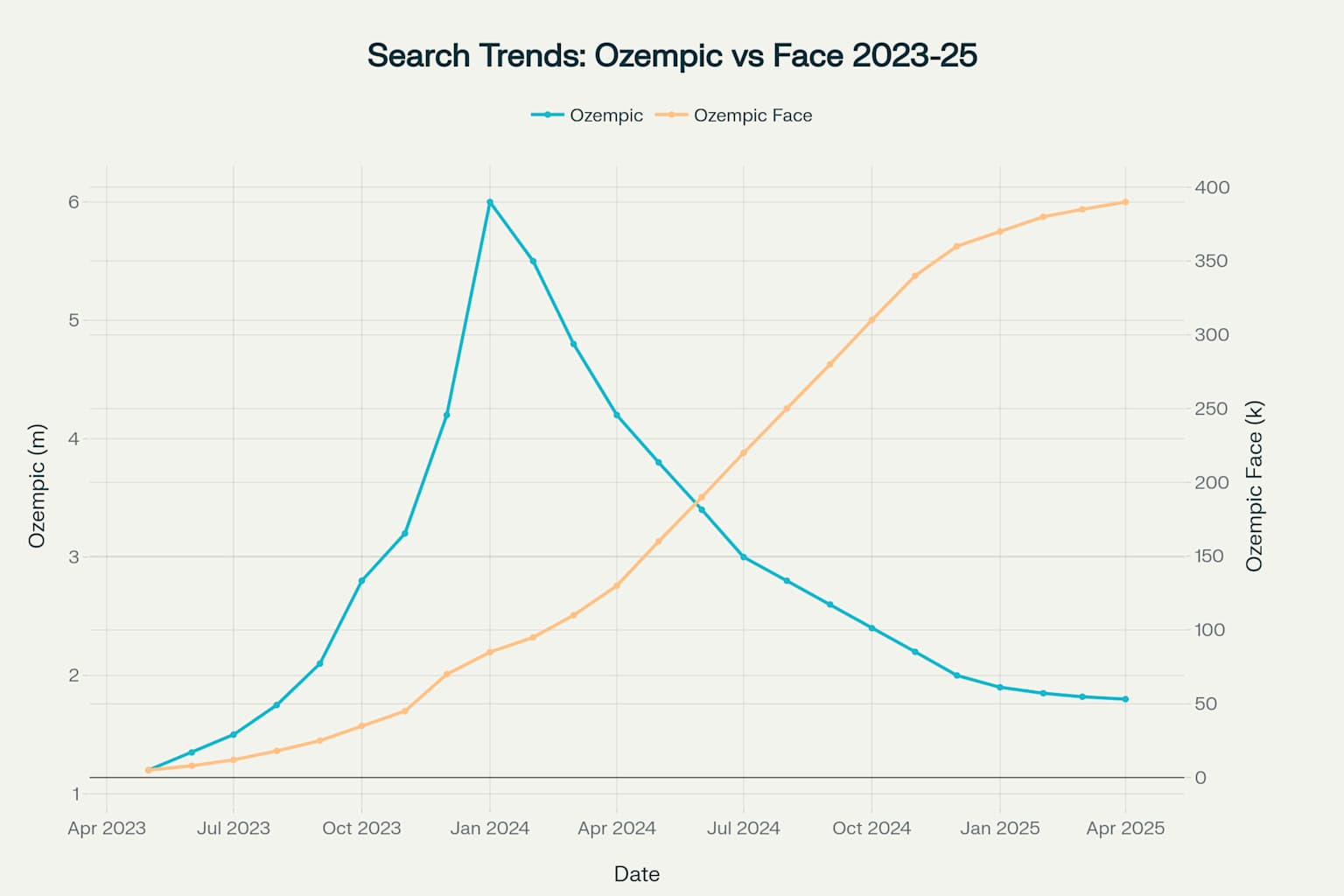
First comes weight loss. Then comes the moment every patient dreads: "Wait, can I get my old face back?" — A recent McKinsey survey of 174 U.S. aesthetic clinics revealed two-thirds of GLP-1 patients were first-timers, driven by concerns about the viral side-effect Hollywood has gleefully nicknamed "Ozempic face."
The problem is that rapid weight loss causes facial skin to lose its elasticity, resulting in hollow cheeks, sagging jawlines, and prematurely wrinkled necklines.
Predictably, the internet doesn’t miss a chance to convert panic into clicks.
Monthly searches for "Ozempic face" have soared, growing nearly 20% every month from April 2023 through April 2025, marking one of the sharpest, most enduring spikes in aesthetic-related internet search history.
But the part of McKinsey's analysis that really caught my attention was how 61 percent of these aesthetic newcomers lost between 11 and 30 percent of their body weight. This is exactly the range of weight loss that Wegovy and Mounjaro consistently delivers.
Clearly, this isn't an isolated problem affecting just a niche group or an unlucky few. Instead, this data signals an emerging "new normal," in which large numbers of post GLP-1 patients will be actively seeking solutions for tightened, smoother skin and restored facial volume.

The real nugget here is figuring out how to treat these concerns effectively and seamlessly for a patient base already stretched thin by ongoing treatment costs.
I imagine the current approach where individual patients are bouncing from med-spas to dermatologists to surgeons, paying piecemeal, and receiving conflicting advice is probably unsustainable.
The smart move for a D2C is developing coordinated, evidence-based treatment protocols that guide patients through each stage of their post-weight-loss journey.
This might mean starting with affordable Tretinoin and topical retinoids that stimulate collagen production early on. For deeper facial volume loss, it could mean partnering with aesthetic clinics to help step patients up to fillers at exactly the right time (umm, the filler industry is definitely set to boom).
And that’s why I’m going to keep pounding the table on this one: You have to build a tightly integrated care ecosystem that anticipates and addresses patient needs at every stage. Your value comes from connecting the dots and removing friction. When your patients can count on you to proactively solve their next concern, you create trust, you build loyalty, and you achieve that good ol’ stickiness.
And stickiness always wins.
America’s shopping carts are changing — Especially if you or someone you know is on a GLP-1 medication. Households with at least one GLP-1 user trim grocery spending by about 5.5% within just six months. With the average monthly grocery budget around $630, that’s a tidy $416 saved annually per household.
Certainly not pocket change.
What vanishes first from these slimmer shopping baskets? Supposedly, it's the calorie-packed indulgences like chips, sweets, bakery items, and cookies (the good stuff). All down roughly 7–11%. Patients claim they're dutifully swapping sugary snacks and greasy fried foods for celery sticks and apples.
Plausible, maybe.

But forgive my skepticism. Humans notoriously inflate their healthy habits, especially when taking meds branded as “game changers.” Odds are, they're probably not trading Oreos for carrots, they're just eating less of everything.
Yet even if these virtuous self-reports are suspect, the commercial impact on big food is undeniable. Kellogg’s recent Q1 earnings were….grim:
Their CEO carefully frames this as a consumer shift toward "health and nutrition," a positive spin worthy of our admiration. Sure.
Now here’s my theory: with one in eight American adults now on GLP-1s, reduced appetites and smaller snack cravings likely ravaged Kellogg’s quarter.
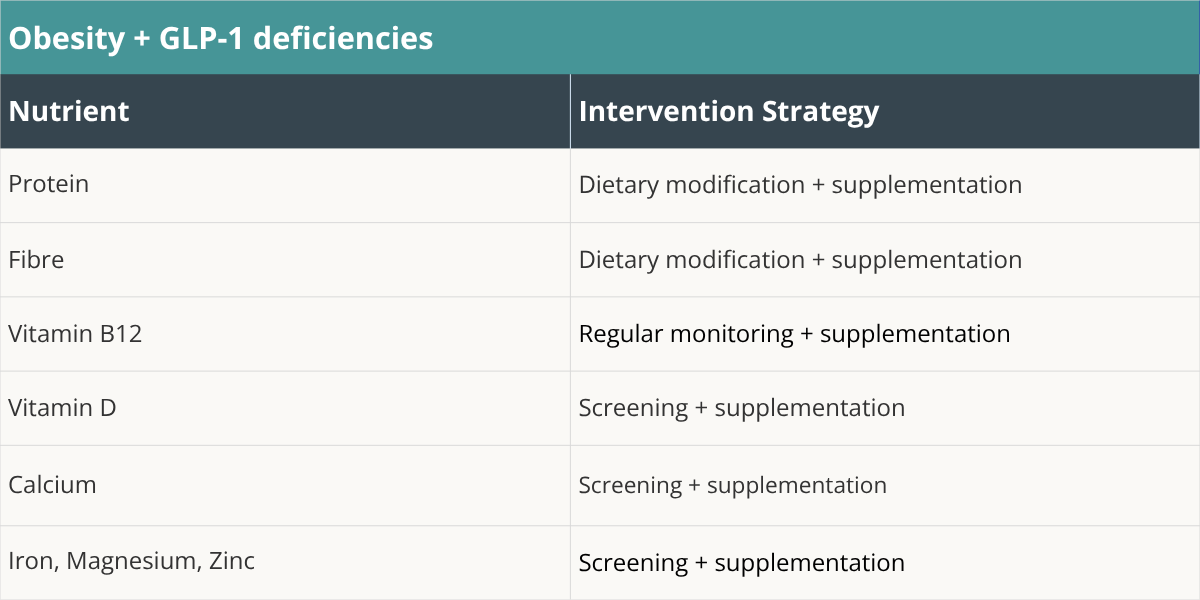
And this, in my view, explains precisely why the cereal giant is swiftly pivoting focus. Cereals—like Kashi GO, Special K, and Mini Wheats—are now prominently marketing their high protein and fiber content. The reason is because GLP-1 usage creates unintended nutritional gaps in protein, fiber, and essential micronutrients.

Kellogg is probably positioning itself as a solution to these deficiencies instead of being a ‘Gr-r-reat’ snack anymore.
If you’re a founder, you should be paying attention here. If eating habits are fundamentally changing because of GLP-1s — and the numbers say they are—then nutritional gaps will inevitably follow. Left unaddressed, these deficiencies can worsen side effects and ultimately cripple retention.
The opportunity is straightforward. Provide simple, thoughtful supplementation and fortified food products tailored to these gaps. I haven’t seen anyone do this well, yet.
To get you started, here's a helpful shortlist from the American College of Lifestyle Medicine that points out the nutrients you need to fix for obese patients taking GLP-1s.
Why BMI actually works for measuring body fat — People love to bash BMI. "It's outdated!" "It doesn't know the difference between fat and muscle!" Yep, fair points. BMI definitely has its limits. But what if it's actually doing its job way better than we give it credit for?
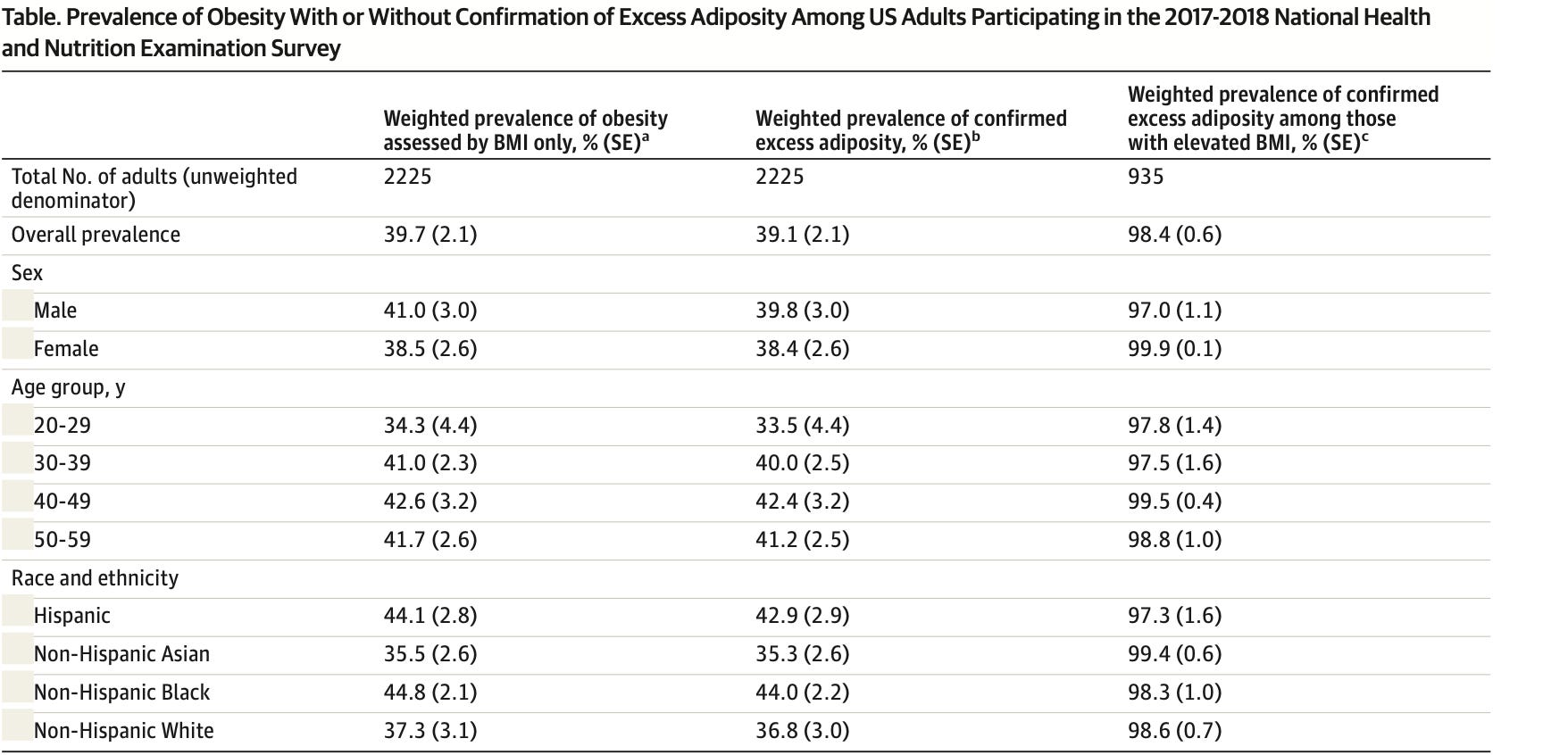
New research published in JAMA tested if BMI alone could accurately spot excess body fat, the real villain in obesity-related health risks, by comparing it against detailed body scans (DEXA) and waist measurements. Using data from thousands of US adults in the NHANES survey (2017-2018), they found that:
98.4% of people classified as obese by BMI actually had excess body fat.
Results held steady across all ages, genders, and ethnicities.
In other words, BMI alone is remarkably accurate at identifying people who genuinely carry excess body fat. This is exactly the group doctors are concerned about when diagnosing obesity.
Here’s what I think:
You don’t need waist-to-hip ratios or expensive scans as your frontline obesity screening tool. BMI alone is quick, cheap, and highly accurate.
If your business is built around highly personalized care, like premium health assessments or specialized wellness platforms… adding waist-to-hip measurements might be helpful to add more nuance…but BMI is still pretty damn good.
🔎 Policy Watch
🇮🇳 Patent battles surrounding Novo Nordisk's semaglutide are intensifying — especially in India. These disputes revolve around two patent types: primary and secondary.
Primary patents protect the fundamental drug invention—essentially, the core molecule itself. For semaglutide, these primary patents expire around 2026 (in India).
But then pharma layers up secondary patents, which are smaller incremental additions, such as tweaks to dosage, new formulations, improved delivery devices, or manufacturing processes.
While individually these changes might seem minor, strategically stacking them allows Novo to build a protective "wall" around their product, potentially keeping generic companies out of the market as far out as 2033.
India’s Dr. Reddy's Laboratories is directly challenging these secondary patents, claiming they're predictable, incremental variations—known as "evergreening"—rather than meaningful innovations. If successful, this challenge could dismantle Novo's patent "wall," and allow much earlier generic entry into the Indian market.
This will make semaglutide available at a much, much cheaper cost and will likely cause rapid market erosion for Novo.
Meanwhile, the Delhi High Court has already permitted Dr. Reddy's to export semaglutide to countries where Novo Nordisk does not hold patent protection. These countries include Bangladesh and Laos and are classified as least developed nations by the United Nations, that benefit from exemptions to international pharmaceutical patent regulations.
📡 Regulatory Radar
Straight out of breaking bad — Honestly, I didn't realize how big the underground peptide market had become until I clicked into a Discord server where people openly discussed using retatrutide, an experimental peptide still only in phase 2 clinical trials.
Retatrutide targets GLP-1, GIP, and glucagon receptors simultaneously and has gained serious attention because early studies suggest it can trigger dramatic weight loss, potentially more than 20% body weight. Enough to blow past Mounjaro.
What shocked me was that despite retatrutide only being in Phase 2 trials, meaning we’re still far from fully understanding its safety profile, people were casually sharing their experiences sourcing it from completely unregulated, anonymous online vendors.
They're literally self-administering substances without quality assurance, or even clarity about what's actually in their vials. As I read through their conversations, all I could think was… what the ****?!
Are people that desperate for weight loss that they'll gamble with completely unproven compounds?
When I dug a little deeper, I discovered Finnrick, a startup backed by heavy hitters like Naval Ravikant. They've positioned themselves as a watchdog in the market by independently testing vendors for purity and quality and publishing safety scores.

They even allow individuals to submit their own samples for testing, basically becoming the peptide world's answer to those festival drug testing tents.
I'm honestly pretty conflicted about the whole idea. On one level, Finnrick is doing something clearly valuable. But the fact that a service like this even needs to exist screams just how badly this market has spiralled out of control.