

Watch on Youtube • Listen on Spotify
The best podcasters have this quality of asking really good questions, and what I’m learning is that the way to do that is to ask from a place of genuine curiosity, no matter how “dumb it sounds. I’m slowly getting better at it, I think, by getting over the fear of recording and putting the episodes out into the ether.
The other thing about podcasting is that sitting one-on-one with world-leading experts is an insane way to learn. I kind of wish I did it sooner, because I’m absorbing information at hypersonic speed, and I’m hoping to pass those insights on to you.
That brings me to Dr. Beverly Tchang, who is a triple board-certified obesity medicine specialist, endocrinologist, and associate Professor of Clinical Medicine at Weill Cornell. I’ve followed her work for a long time, and she’s one of the few expert clinicians who thinks commercially, because she also advises Ro.
Our conversation went on for over an hour, and it could’ve easily gone longer. I urge you to listen in full, and here are three insights that I think will have a tangible commercial impact on where this industry is heading.
But first, this post is proudly brought to you by Sacher AI.

Retention is the business problem every D2C weight-loss platform is trying to solve right now. And increasingly, teams are betting on AI coaching to fix it. But the problem is that without genuine clinical depth and experience in this space, you end up with one of two outcomes: an AI agent that plays it so safe it’s useless, or one that crosses lines you didn’t know existed.
Either way, retention doesn’t improve.
Sacher AI is a leading AI consulting firm that I point people to because they’ve solved both sides of this problem. They’ve analyzed thousands of real patient conversations and built systems that know how to retain patients and keep them engaged. Their team includes clinicians who’ve published peer-reviewed research on AI in obesity care.
If you’re building patient-facing AI in this space, talk to Sacher AI first.
1. The maintenance problem
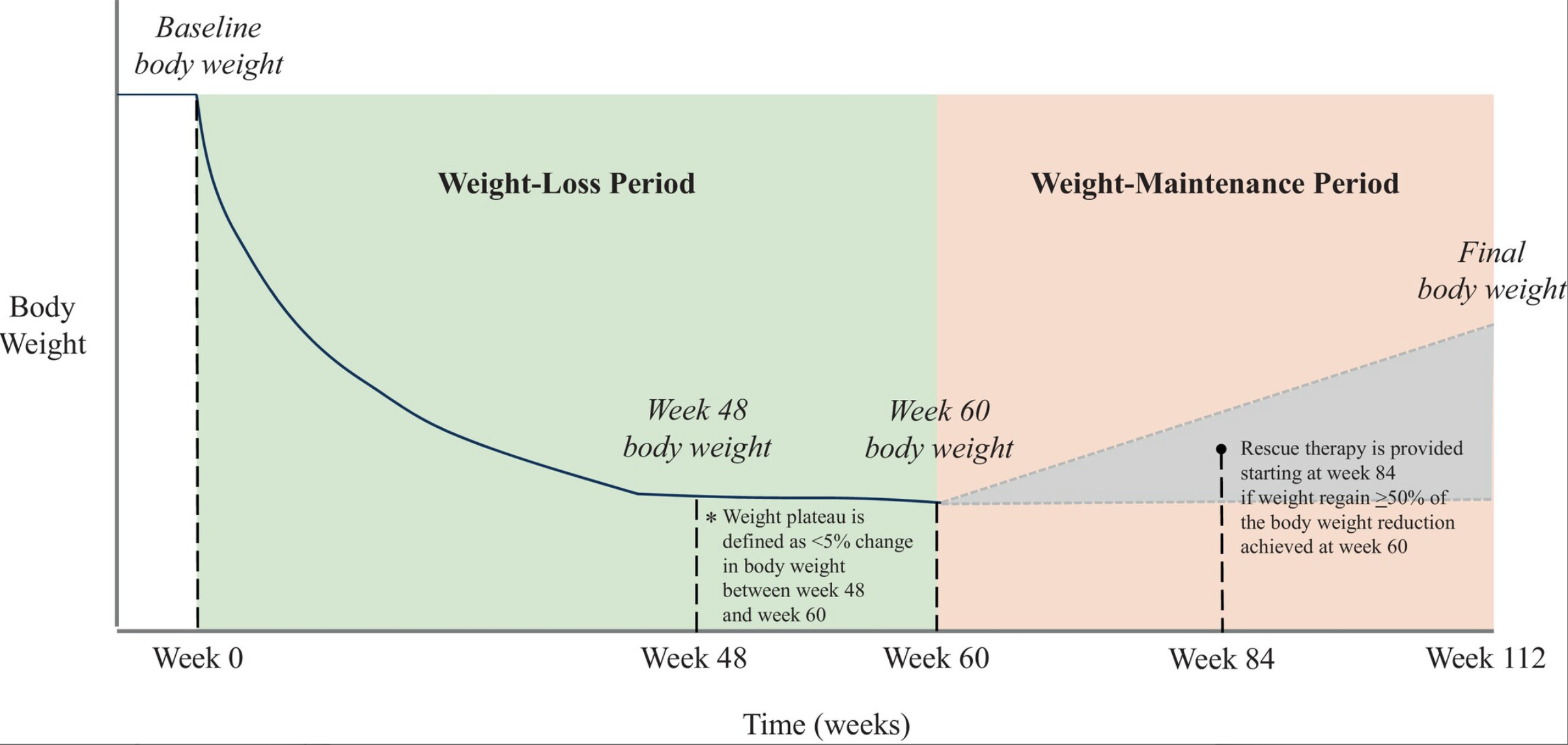
I’ve noticed the conversation in the most popular GLP-1 subreddits shifting from “how do I lose weight with GLP-1s” to “how do I keep the weight off,” which means we’re entering the next battleground for telehealth platforms: retaining weight-loss maintenance customers.
Weight-loss maintenance starts once the active weight-loss phase is over and the patient’s goal shifts from losing more weight to preventing weight regain. Many providers think that both the weight-loss and weight-loss maintenance phases require the same level of hand-holding, so they’re promoting wrap-around care services for both phases. But Dr. Tchang thinks this is the completely wrong approach for retention and lifetime value:
“In weight-loss maintenance, people just don’t want to feel like they are in a program or that they’re patients still, that they’re being medicalised. They just want to feel normal.”
This is such a powerful clinical insight, because it means maintenance is a fundamentally different product to weight-loss.
Even though patients are often taking the exact same drug at the same or slightly adjusted doses, what changes is how they want to buy it and the level of care associated with it, and I think this explains why many customers switch and migrate to simpler, more transactional services where they can get their medication without the ankle-monitor and simply get on with their lives.
For providers who want to keep these customers, there are two obvious levers that would have a dramatic impact on both contribution margin and lifetime value.
The first is scaling back the check-ins and clinical surveillance, which is both a cost-saver and exactly what patients are asking for.
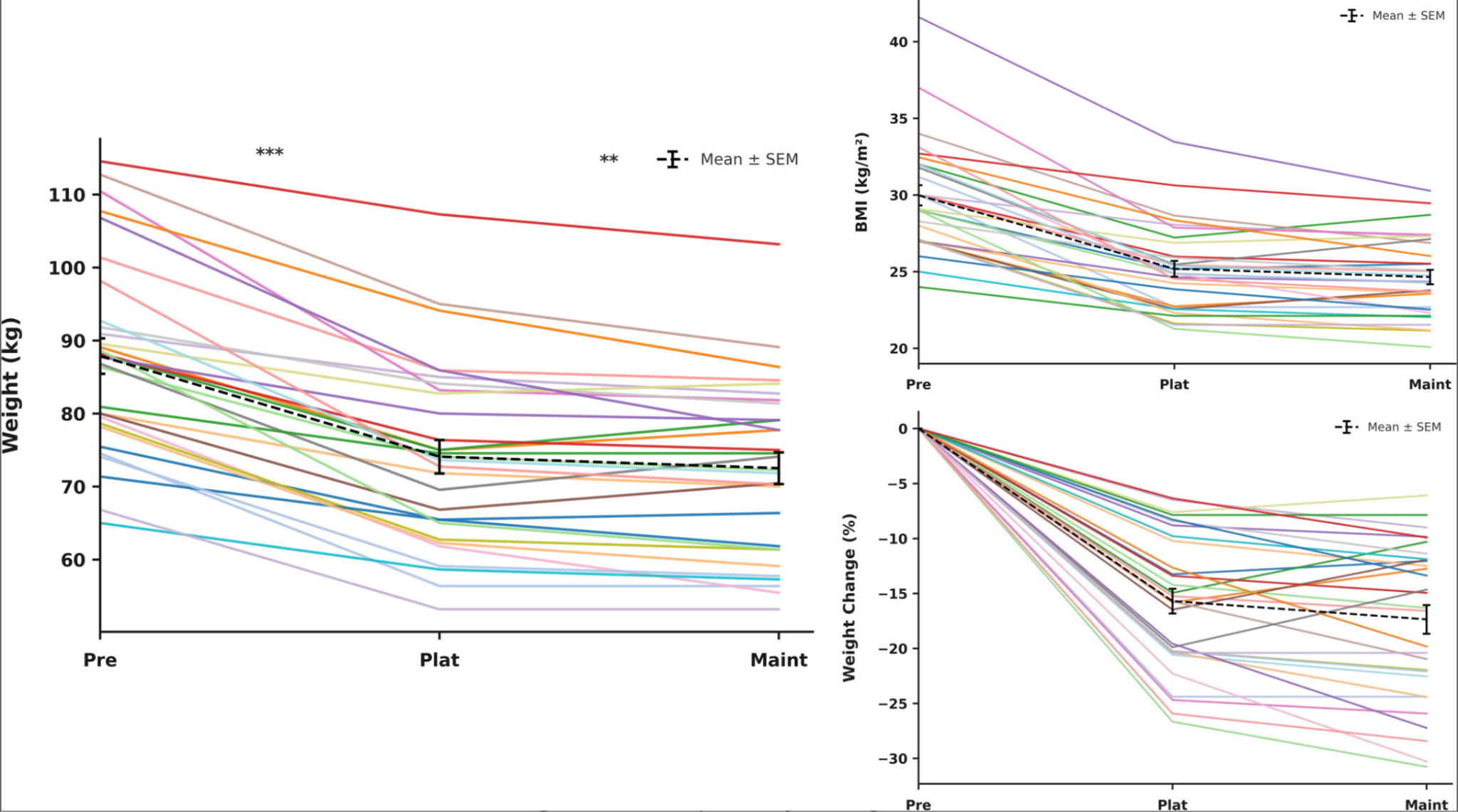
The second lever is injection frequency, extending pen usage through off-label dosing to stretch what was a monthly supply into six or eight weeks so that the patient injects less often and pays less. There is increasing evidence that this approach works, with a recent study publishing the benefits of infrequent dosing as a method for maintaining weight loss.
Both levers would create a product that feels less like ongoing treatment. And if Dr. Tchang is right that maintenance patients just want to feel normal, I think this is exactly the kind of low-friction experience that would keep them from dropping off.
2. Why are we waiting for people to get sick?
A patient’s BMI determines their eligibility for GLP-1s, and those cut-offs come from clinical trials: BMI of 27 for patients with comorbidities and BMI of 30 for those without. So, in practice, a patient must gain enough weight to cross the BMI threshold before they can access treatment.
But what about those people just on the cusp of eligibility, or those who’re trending dangerously upward in weight but don’t yet meet the BMI criteria?
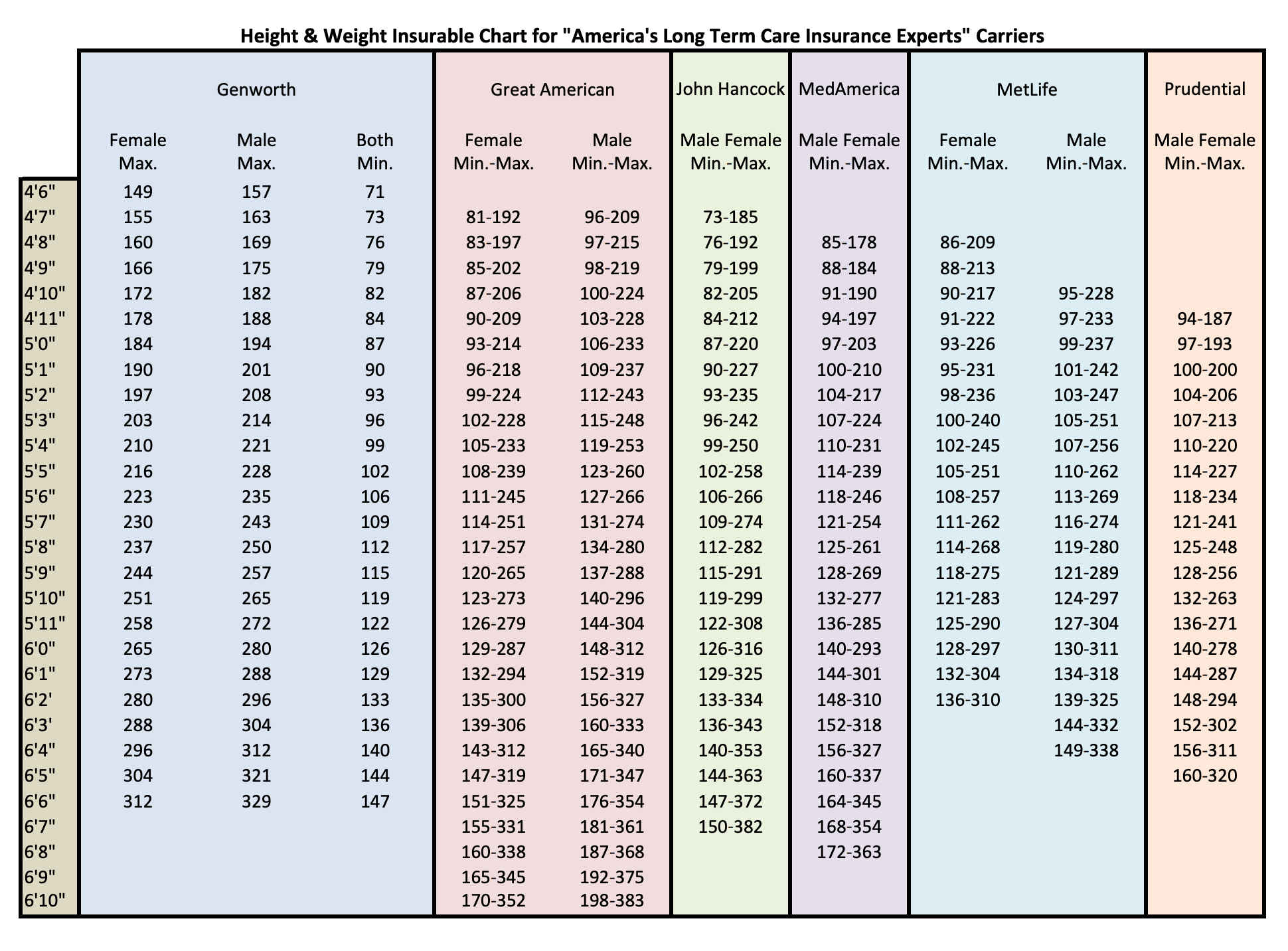
Before BMI became the standard, MetLife — one of the biggest US life insurers — used height–weight tables that flagged any deviation from your baseline. Someone who’d been 66 kilograms their whole adult life and had slowly (or suddenly) put on 20% would get attention from a medical provider, because clearly this is a signal that something is happening metabolically.
The problem now is that we’ve resorted to using BMI everywhere, and BMI is only a snapshot in time. It tells you where someone is, not where they’re heading, so that same person, whose body is clearly changing, gets nothing because their number still reads as ‘normal.’
As Dr. Tchang put it, “why would you wait for someone to gain even more weight before you intervene. That sounds crazy?”
This is where microdosing becomes a very interesting concept.
The definition of microdosing is a minefield and we discuss this in the podcast, but “sub-therapeutic” dosing could be enough to stop weight creeping above the “overweight” and “obese” BMI thresholds without needing (or becoming eligible for) the full therapeutic dose.
Dr. Tchang does this in her clinic already with slower titration and in-between doses, tailored to the individual.
The conundrum of course is that healthcare professionals will be demanding evidence that this approach works. And yet, Dr. Tchang is very blunt about this:
“The amount of money it takes to show that this intervention prevented XYZ in a particular population is just too large. Too many uncertainties and too many variables. No one is going to invest in that clinical trial.”
So, we’ll probably never get the randomized controlled trial that proves early low-dose intervention prevents obesity. But there is biological plausibility, and as Dr. Tchang puts it:
“We are different people every decade. Your body changes through every stage — and the idea that a single BMI number determines whether you deserve treatment ignores everything we know about how bodies actually work.”
Her approach is to be transparent about the uncertainty and let the patient decide: “As long as we’re honest that we have no evidence, if this is still a risk that [a patient wants] to take on, we can do that together.”
I personally think we’re heading toward a world where treatment thresholds come down, and I’m a strong advocate for clinicians with real expertise pushing those boundaries rather than waiting for guidelines to catch up.
Of course, players like Noom and Hims & Hers have already lowered their BMI thresholds and use a microdosing strategy for these customers — and it’s only a matter of time until we see this strategy writ large in the cash-pay channels.
3. Is it time for over-the-counter GLP-1s?
I want to come back to something Dr. Tchang said that I’m still chewing on.
She thinks we need an over-the-counter GLP-1 to really make a dent in the obesity epidemic, and while most of her colleagues would balk at that (as I did), her reasoning is hard to argue with.
First, we already have OTC obesity medication. Orlistat, sold as Alli since the early 2000s, has a terrible reputation as a weight-loss medication because it rarely works, but Dr. Tchang’s point is that it there is precedence for doing this already, despite those drugs being ineffective:
“I don’t think of Orlistat as an obesity medication anymore because it doesn’t really target the root cause of obesity. No study has shown that people with obesity hyper absorbed fat from their diet. That’s not part of the pathophysiology.”
And yet, if a medication is approved for OTC sales, it has already cleared a safety threshold, and the consumer doesn’t need to parse clinical trial data or find a willing prescriber. The safety question is answered by the fact that it’s on the shelf.
“If it’s over-the-counter, that means it has to be safe. You check that box automatically when that bottle is right there at the checkout.”
And Dr. Tchang’s argument for why this matters is about who we’re actually trying to reach. It’s not the patients already in the system and it’s not the people on her clinic waitlist or browsing Hims. It’s the people who will never enter the medical system at all.
“That’s where our non-patients are. People who are not in the medical system, people who don’t have access to doctors like me. They’re just looking at feeds and reels and ads and what their friends are buying. They’re getting their information from marketing.”
Dr. Tchang calls this space “primordial care” — the stage where people engage in their health journey before they engage in the healthcare system and obesity has always lived there.
“For decades we’ve said it was a lifestyle problem, and it’s always existed in this supplement space. It’s never really entered the medical system. . . . It’s a muddled game between industry and payers, consumers, prescribers, patients. Who’s paying for what and who’s actually getting the service? It’s very messy.”
OTC potentially cleans all of that up, and in her view, Dr. Tchang predicts that obesity will be solved:
“It’s going to be driven by Gen Z and Gen Alpha in combination with an over-the-counter medication. And that’s how we’re going to fix this.”
I personally think the lowest starting doses of semaglutide and tirzepatide could feasibly be sold over the counter with pharmacist oversight, much like how lower doses of sildenafil and statins can be dispensed across UK pharmacies without a prescription.
For the stronger doses, a prescription would definitely be needed.
It’s funny because two decades ago, the same conversation was happening with statins. The population-level cardiovascular benefits were so clear that making them more accessible seemed obvious. And yet we still haven’t fully got there, largely because the media demonised statins despite their life-saving potential. Whether GLP-1s follow the same trajectory or break through faster remains to be seen, but if a clinician like Dr. Tchang is openly advocating for OTC access, it’s certainly on the minds of public health experts too.
Founding memberships are open. Get exclusive access to paid research, white papers, and the kind of analysis that actually moves the needle on your GLP-1 business decisions.
I am also taking sponsorships for Q3. Drop me an email by replying to this post.
**The views, opinions, and recommendations expressed in this podcast and essay are solely my own and do not represent the views, policies, or positions of any other organization with which I am affiliated. This content is provided for informational purposes only and should not be considered medical, legal or investment advice.**
