

After recording six episodes, I have a much clearer picture of what I want this podcast to be. These conversations I’m having with world health experts contain so much rich, multi-layered context, and the purpose of the pod is to make that information as accessible and as easy to reference as possible.
I also think that in the next three to six months, fewer of you will listen to podcasts directly, and more of you will ask your AI agent to brief you on what matters. I want to be ready for that. So, starting today, there’s a button below that lets you pull this episode directly into Claude for a summary and analysis, and soon, I’ll have a way for your personal AI agent to do the same from your phone.
Now, on to this week’s guest. Lord James Bethell is a former Health Minister who served as Minister for Life Sciences in the UK during Covid. He sat on the IPPR Commission that called the UK “the sick man of Europe” and now chairs Business for Health and works closely with the private health sector through his advisory role at Oviva.
In this fascinating conversation, we zoom all the way out to the big picture, covering the population-level impact of GLP-1s, how government ministers are thinking about the direct-to-consumer market, and the widening gap between what the NHS aspires to and what it actually delivers.
There are so many excellent snippets, and I have chosen three of them to expand on here.
•Watch on Youtube • Listen on Spotify
1. Do GLP-1s Extend Healthspan?
Last month, the Office for National Statistics published data showing that healthy life expectancy (years of life spent in good health) in the UK had fallen to its lowest level since records began in 2011. Men can now expect to spend 60.7 years in good health, while the average for women is ever so slightly higher at 60.9 years.
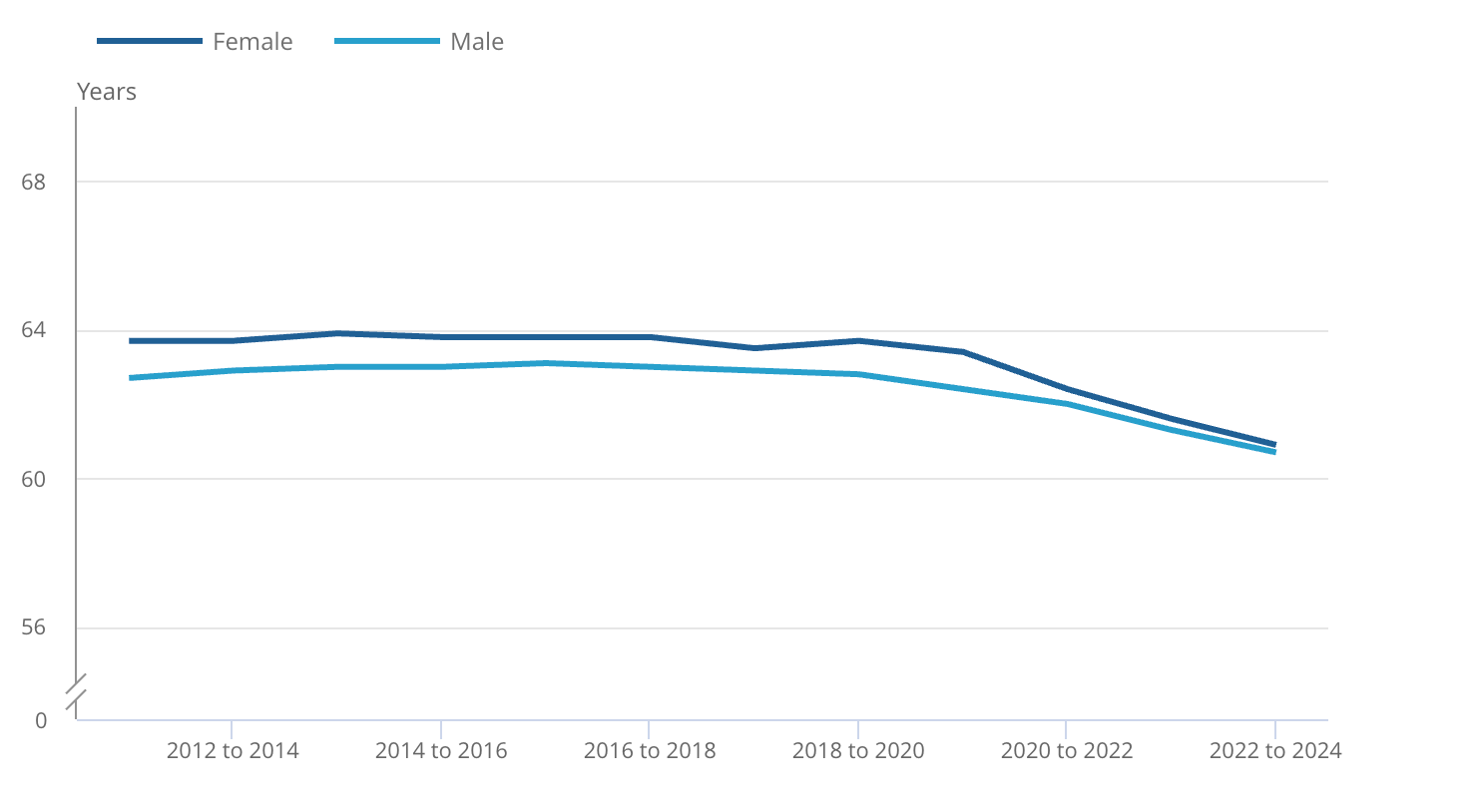
Based on the UK population average, at 33, I can expect roughly 27 more years of good health before I’m zapped by a chronic disease or a bout of sickness that takes me out of work and makes me more dependent on the NHS. And then what? The average UK male lives to around 79, so if the good health clock runs out at 61, that’s 18 years I’m most likely living as a burden to the state.
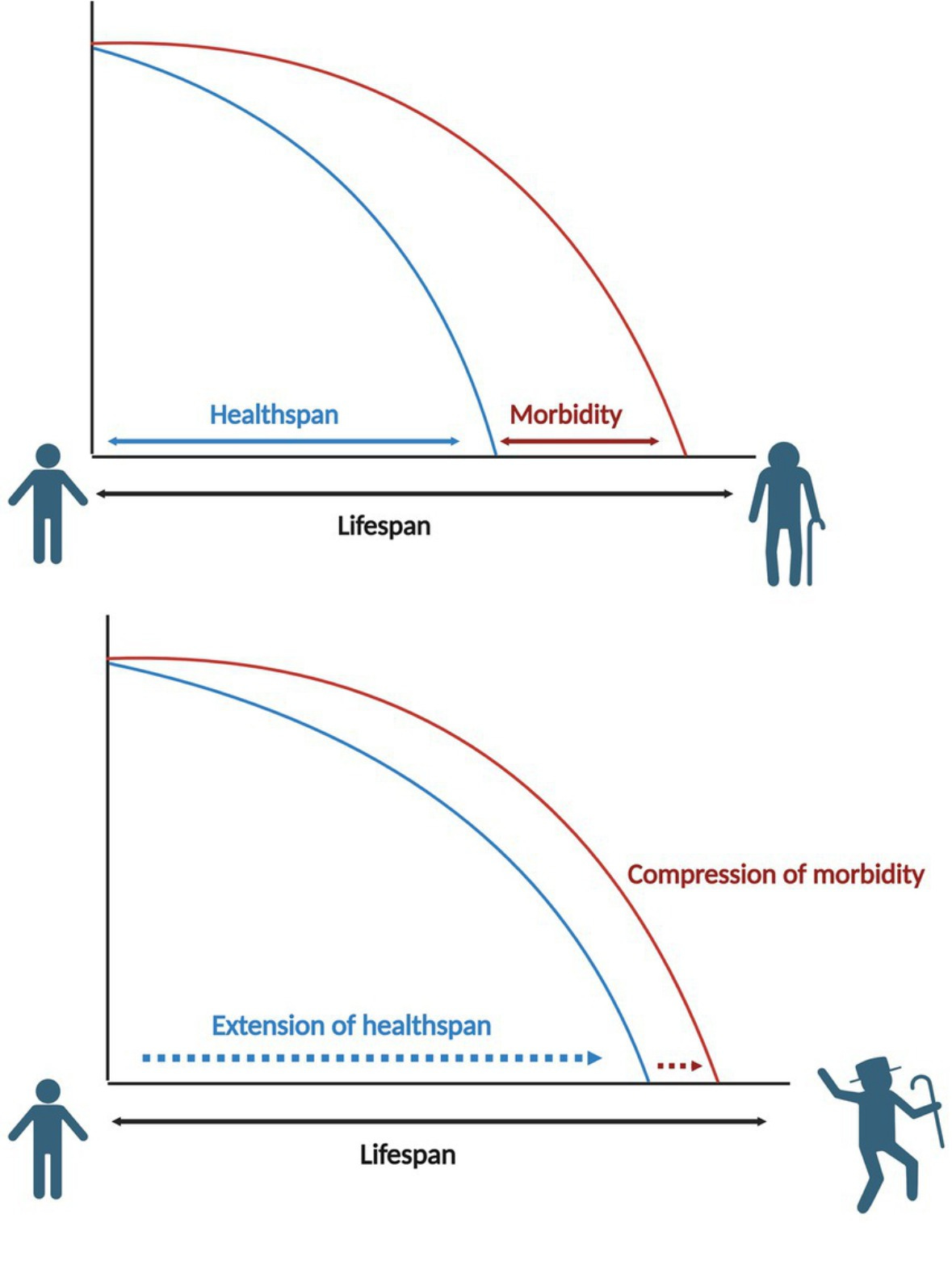
The only way to reasonably fix this is to keep people healthy for longer by preventing the onset of disease (morbidity) as long as we possibly can.
But the political will for prevention has never truly landed in Whitehall, because the incentives are misaligned. The work on morbidity-prevention needs at least a twenty- or thirty-year time horizon, but the government thinks in a five year cycle.
When I put this to Lord Bethell, he didn’t sugarcoat the consequences:
If we have people living longer but spending longer in poor health, it costs the country a fortune. Not the NHS, but the Exchequer [treasury]. It costs our businesses and communities because they’re not contributing. I don’t know how your generation is going to pay off the national debt.
Neither do I. And the picture is particularly bleak when you consider that deaths are now exceeding births, which means the young, healthy people who are supposed to be funding this mess with their taxes are a shrinking population.
Basically we’re becoming like Japan, with a population that skews elderly, but we Brits are much sicker.
However, there are some reasons to be cautiously optimistic with the arrival of GLP-1s. Similar to statins, they can slow the effects of chronic disease that can disable you and limit one’s physical or mental functions. This is known as secondary prevention, which means easing symptoms of chronic disease while not forestalling morbidity. Secondary prevention is the first test a drug has to pass before it’s considered for primary prevention, and therefore as a healthspan-extending drug.
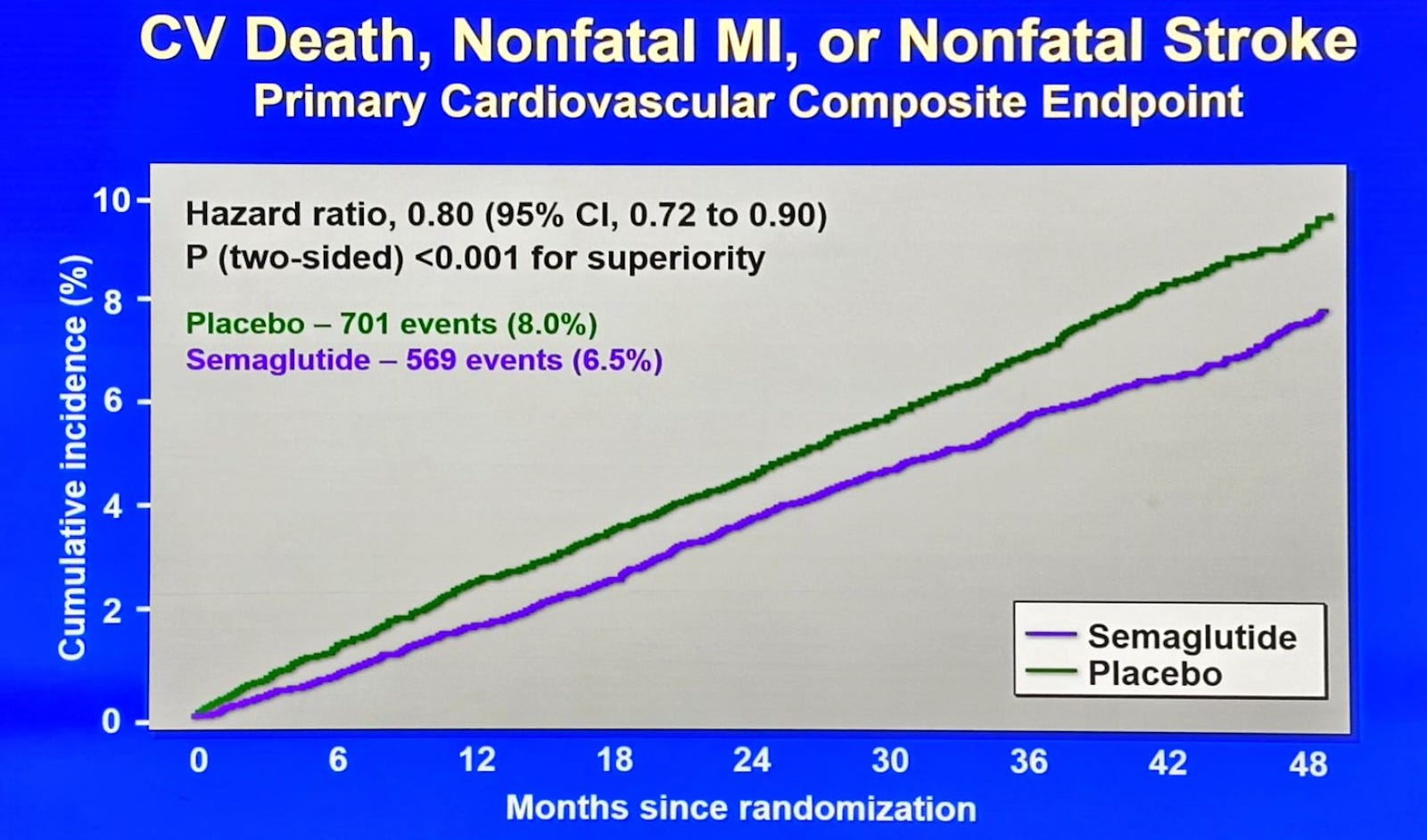
In the SELECT trial, semaglutide reduced major cardiovascular events (like heart attacks, strokes, and deaths) by 20% in adults with obesity and established cardiovascular disease, independent of weight loss, which means the drug is most likely exhibiting anti-inflammatory effects on the cardiovascular system.
On a population level, for every 67 people treated over a 3-year time frame, one person will avoid a heart attack, stroke, or other cardiovascular-related death.
This efficacy metric is called the number needed to treat (NNT).
At first glance, the NNT for GLP-1s is less impressive than the NNT for statins, which is ~20/25 ( statins are also much cheaper). But statins only prevent cardiovascular events.
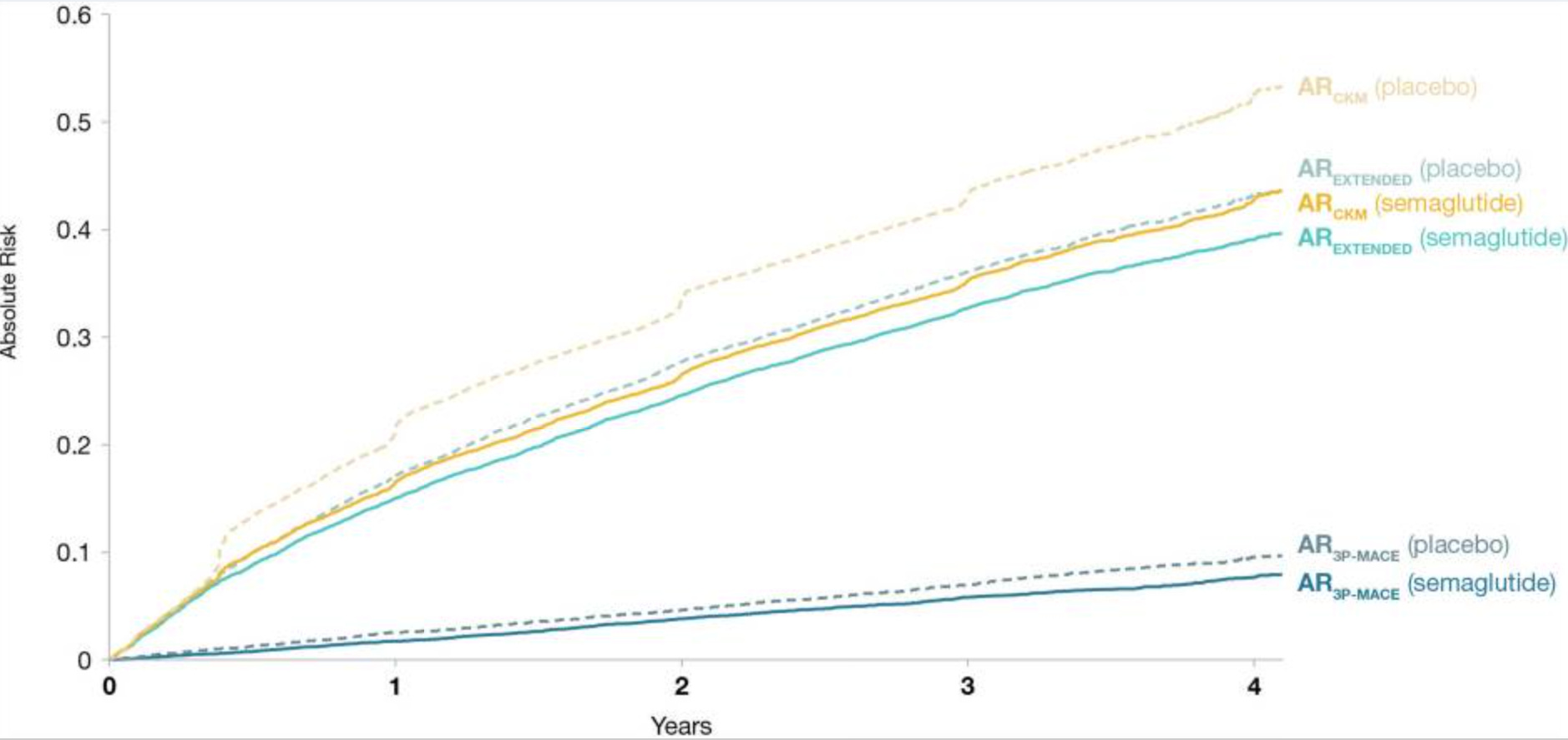
GLP-1s prevent cardiovascular events and produce significant weight loss, which independently reduces the risk of type 2 diabetes, joint disease, sleep apnoea, and several cancers. Statins, by contrast, do one thing: they lower cholesterol to reduce cardiovascular risk. GLP-1s do that and fix the underlying metabolic dysfunction driving much of modern chronic disease. So an NNT of 67 is a crude measure here, capturing only one benefit of a drug that is producing several.
Across the full range of cardio-metabolic conditions it prevents, the real NNT is likely much smaller.
But what about primary prevention? Primary prevention means stopping the disease from developing in the first place, in people who are currently healthy or at-risk but asymptomatic. It is a far more interesting and commercially important question on whether GLP-1s can deliver on this, and the argument I want to propose is comparing the primary prevention effects of statins with GLP-1s.
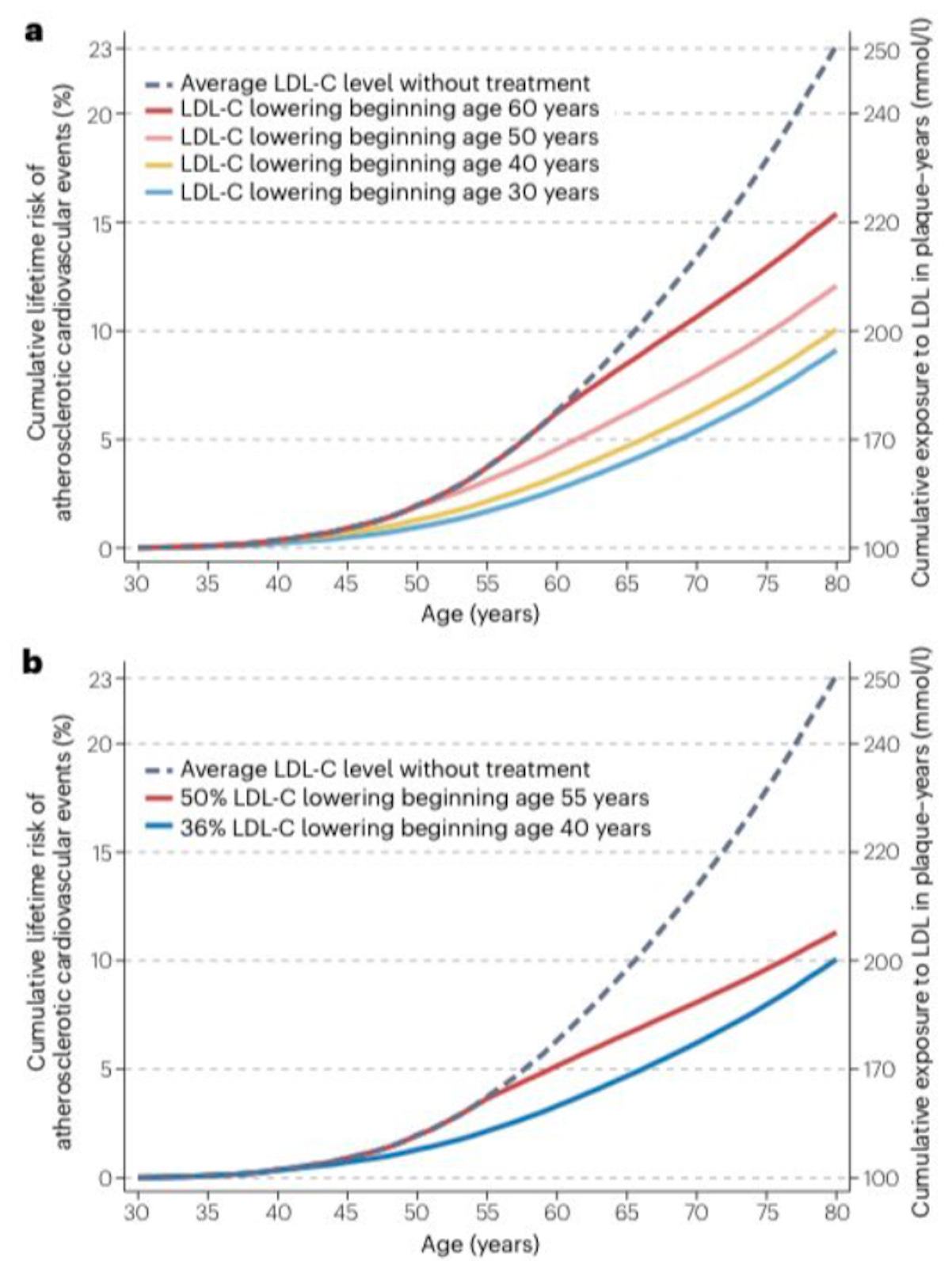
Statins are miracle drugs because they can prevent cardiovascular disease in high-risk people, and there is a growing consensus that the cumulative lifetime exposure to LDL-C is the risk factor that most determines your cardiovascular risk.
Therefore, starting statins earlier in moderate to lower-risk people, including people in their 30’s before the plaque has had decades to accumulate produces compounding benefits that lowers lifetime risk of a major heart attack, stroke or death.
GLP-1s have not shown any benefit for primary prevention, because those studies don’t exist yet, and if they did, the first step would be identifying people with obesity at high risk of developing cardiovascular disease and trialing prevention in that scenario.
But if cumulative exposure to a single risk-factor justifies early intervention at an earlier age with statins, what does cumulative exposure to LDL, triglycerides, blood pressure, blood glucose, systemic inflammation, and visceral adiposity imply for a drug that lowers all of them simultaneously?
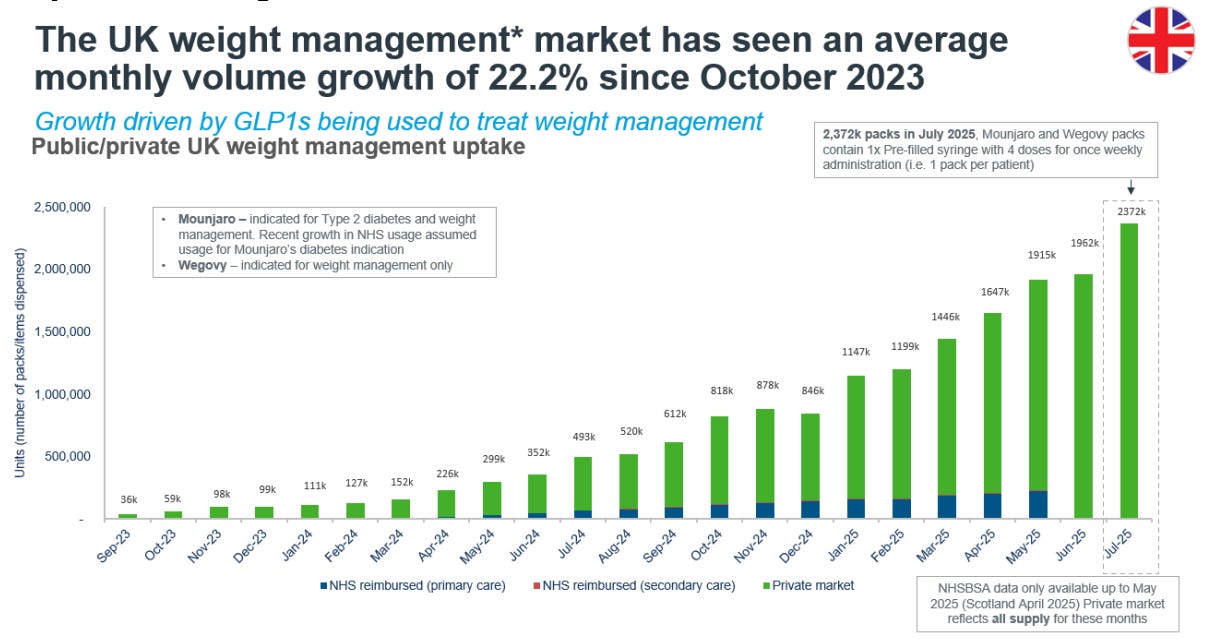
2. The UK Private Market Is Scaling
The reaction from people inside the NHS to the direct-to-consumer GLP-1 market is, overwhelmingly, one of disdain and distrust. I’ve heard many NHS clinicians refer to online providers as “cowboys,” which is interesting given that those cowboys are processing upwards of 100,000 prescriptions per week, roughly 2.5 to 3 million patients a year, at a scale the NHS has shown no ability or willingness to match.
What’s actually happening is that the monopoly on the patient relationship is dissolving away from the traditional gatekeepers of health, and when power structures change, the obvious reaction is one of visceral anger and frustration. More importantly, the private GLP-1 market has expanded the willingness to pay for healthcare in general.
Lord Bethell puts it this way:
It completely reboots people’s expectations about how they’re going to engage in their own health. If you’ve struggled with your weight for years and suddenly you’ve lost five kilos, ten kilos, and you’re on a different trajectory — my goodness, that’s tremendously good value. So maybe you start thinking, maybe I’ll just pay for my Covid vaccine, or maybe I will take a Shingrix vaccine, or maybe I will do any number of interventions that will modify my risk.
GLP-1s were simply a wedge into the broader commercialization of healthcare. What we’re going to see in the next two to three years is people no longer waiting for a general practitioner (GP) to organise a blood test or recommend a treatment because they’ll just go to the private market, pay, and move on.
The common pushback from NHS people is that privatisation perpetuates a two-tiered system and exacerbates inequity. My two responses to that are: first, people going private are in fact relieving pressure on the NHS, which is a net good.
And second, and more fundamentally, the inequity argument assumes there is an equitable system being undermined. Equity, in this context, would mean giving everyone who needs these drugs a genuine shot at accessing them. But the NHS isn’t currently offering GLP-1s at anything close to population-scale, because most of the people going private were never going to get these drugs through their GP in any reasonable timeframe.
3. Privatization Promotes Agency
Right now I’m infected by a mind virus called agency which I picked up from the depths of tech Twitter. If we want people to exercise agency over their own lives — a permissionless, “just do it” mindset — then how? And why do some people exercise more agency than others? I don’t have a clean answer to that.
But I do know this: the NHS is the least agentic system I can think of. The social contract is, as Bethell puts it:
Live your life however you like, no worries mate, just rock up and we’ll put you back together again. Which is proving to be a very, very expensive underwriting exercise by future generations.
The consequences of disengagement are visible everywhere in the system.
Bethell points to missed appointments as a telling example:
The NHS logs hundreds of thousands of ‘did not attends’ every year, and in political focus groups, the frustration with people who skip appointments they didn’t pay for and didn’t fight to get runs surprisingly hot.
When there’s no personal investment in accessing care, there’s no cost to wasting it.
But the system also infantilises the people who do engage:
The culture of the NHS is: don’t believe the patient. If you ask the patient how much they weigh, don’t believe them. What a lousy way to run a health system.
I personally think elements of privatization fixes this. When people pay for their own care, they have real skin in the game, a direct incentive to show up, follow through, and take ownership of their health decisions. And once there is ownership, I think agency naturally follows.
Whether the NHS adapts to this shift or continues to resist it remains to be seen, but the direction of travel is that more and more people are already making the choice for themselves, and I don’t see that reversing.
Founding memberships are open. Get exclusive access to paid research, white papers, and the kind of analysis that actually moves the needle on your GLP-1 business decisions.
I am also taking sponsorships for Q3. Drop me an email by replying to this post.
**The views, opinions, and recommendations expressed in this podcast and essay are solely my own and do not represent the views, policies, or positions of any other organization with which I am affiliated. This content is provided for informational purposes only and should not be considered medical, legal or investment advice.**
