

There are fundamental headwinds coming for the US and UK food and beverage industries. Because of GLP-1s, there will soon be ~3 trillion fewer calories consumed in the US, annually.
I wanted to understand how the food industry is thinking about this. From the outside, it looks like GLP-1s are like a meteor hurtling towards this industry.
That is why I was so delighted to speak with Henry Dimbleby. Henry co-founded Leon, the healthy fast-food chain, and helped grow it into a business that was eventually sold for £100 million. He led the UK’s National Food Strategy, and now invests in the future of food as managing partner at Bramble Partners.
He also wrote Ravenous, which I highly recommend if you want to understand how the modern food system has learned to manipulate our appetites.
Our conversation gave me a much clearer way to think about what comes next, and here are the three most important ideas I took away from it.
But first, this edition of the newsletter is brought to you by Embla.
Same Outcomes, Lower Dosage, Lower Cost
If you’re a benefits leader watching GLP-1 costs climb every year, you already know the problem: most treatment plans keep members on the full dose indefinitely. Costs compound, budgets blow up, and you’re left choosing between unaffordable renewals and cutting coverage your employees desperately want.
Embla solves for cost and outcome. The program is built around behavioural support, so members hit strong clinical outcomes on much lower doses, and most of them taper off the drug entirely. The proof is in one of the largest real-world GLP-1 studies to date. Embla members used 55% lower doses, and they lost 16.7% of body weight in twelve months.
Prescribing a GLP-1 is now the easy part. The hard part is delivering long-term outcomes at a price employers can afford. And that’s the problem Embla solves by creating end-to-end programs for benefit leaders who want to solve GLP-1 coverage for their clients.
1. Better Information Doesn’t Mean Behavior Change
I know, on balance, I should not be eating the Froot Loops my fiancée smuggled back from Canada. I know I should be eating my daily Weetabix with a square of dark chocolate and a fistful of blueberries. I know I should do a lot of things that are good for me because, like many of you, I am surrounded by more health information than I could ever reasonably act upon.
However, being well informed doesn’t necessarily mean I’m going to change my behaviour.
Henry Dimbleby believes this is not a personal failing but simply what happens when human appetite meets a food system designed to exploit it. As Henry told me, there has been “an extraordinary change in consumer understanding of health.” Covid made diet feel more directly linked to wellbeing, ultra processed foods moved from a niche debate into the mainstream, and AI made it easier for people to ask basic questions about what they should eat.
But as he put it, “you end up knowing what to do but not doing it.”
The problem is that our appetite has evolved to endure long periods of scarcity, where every ripe berry or dead antelope was a windfall against the entirely realistic possibility that you would not eat tomorrow. Two hundred thousand years of selective pressure has built a brain that lights up like a slot machine when it sees energy-dense food.
The commercial opportunity is, then, to make calorically-dense food saltier, crunchier, sweeter, cheaper, brighter, and more available. Then, find a way to make it taste good but not be satiating, and people will consume a lot of it.
But, Henry’s point is that food-industry executives are not sitting in dark rooms trying to make people sick. It is much more mundane and less sinister. “They’ve just noticed that if you put chocolate in cereal, they sell more,” Henry explains. “They’re following the money.” As the late, great Charlie Munger once said, “show me the incentive and I’ll show you the outcome.”
That was all before GLP-1s exploded onto the scene. And now for the first time in history, we have a technology that can directly weaken the pull of appetite, with Henry coining the phrase that our “evolved appetite is being hacked by these drugs”.
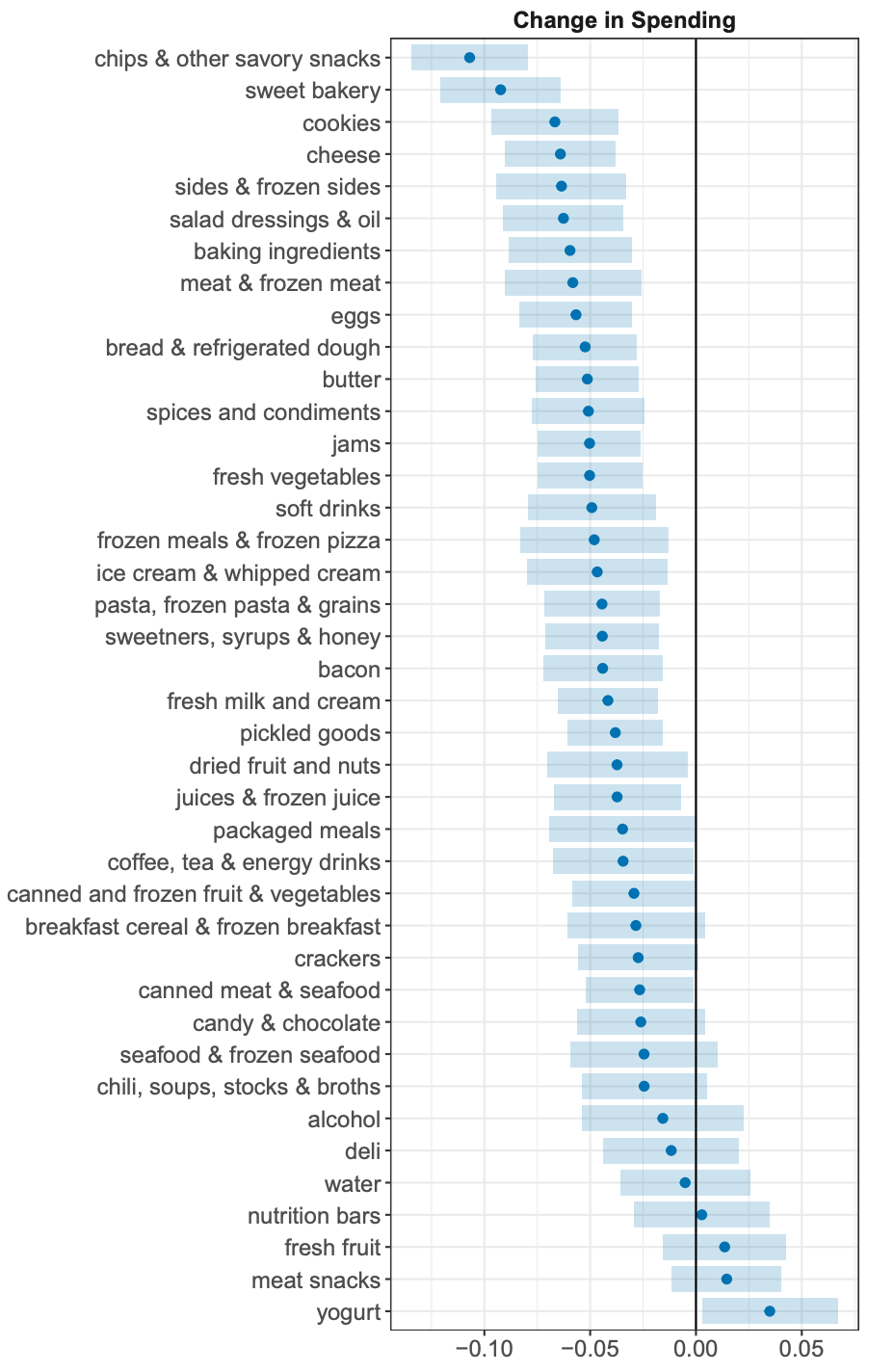
The consequence, in his words, is that “people are going to be able to match that health intent with actually what they eat.” A Cornell study gives us an early look at what that means in real household transaction data, which found that within 6 months, households with at least one GLP-1 user reduced grocery spend by 5.3%, and that decline was concentrated in calorie-dense, processed categories like savory snacks.
2. Consumers Want Value Per Bite, Not Calories Per Bite
I expect that many more millions of people in the US, and eventually the UK, are going to be on GLP-1s in the next few years—accelerated by Medicare Part D coverage, oral options coming to market, and potential NHS reimbursement. When that happens, we can make some forecasts on changes to annual calories consumed per year.
Henry told me that while people are losing weight on these drugs, they eat about 30% less, and in maintenance, he thinks they may settle at roughly 10–15% fewer calories per year.
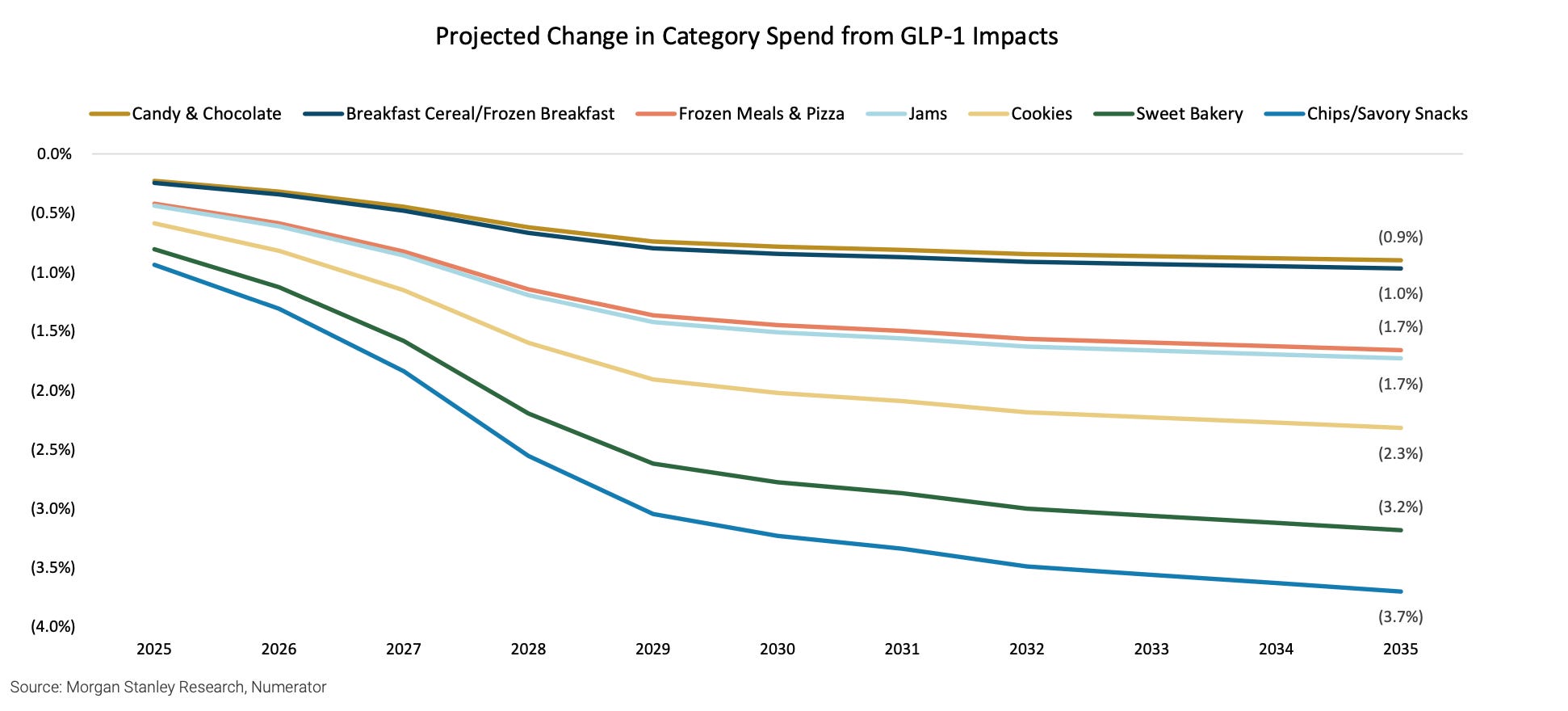
Morgan Stanley modelled similar calorie reductions, and estimated that roughly 55 million US patients will be on a GLP-1 by 2035. Accounting for discontinuations, cycling on and off therapy, and segmenting lower BMI users with lower calorie reductions, they modelled a base case of a 1.6% reduction in annual US calorie consumption, which will disproportionately affect the demand for highly processed foods.
The food industry has never had to contend with a volume-shrinking market. So, how on earth do they respond?
Henry’s answer was threefold:
Take share from competitors.
Sell premium food.
If you’re a supermarket, sell more non-food.
Focusing on point two, if people are eating less, the food they do eat has to justify itself more. Henry’s phrase for this was “value per bite,” where the calories are no longer enough and the product has to come with a healthy reason to consume it: protein, fiber, satiety, muscle preservation, blood sugar, gut health, or some other claim that makes the food seem more useful.

3. Who Is Most at Risk in This New World?
Henry is clear that “most people on these drugs still seem to enjoy food, just in different amounts.” In his view, people will still enjoy going out to restaurants, because, after all, eating food with other people is a social experience, so that won’t change too much. But food-spend is likely to change. People on GLP-1s are likely to go out to eat just as much but spend less per outing.
These changes will lead to some casualties: “Businesses that are basically selling carbs and fat very cheaply will struggle.” Beverage companies are slightly more insulated, because they can innovate to offer zero-calorie products, like Coke Zero or sugar-free Sprite. But, it is going to be much harder to innovate in snacks and alcohol, where cutting calories is much more difficult.
That is why Henry thinks the first casualty may be the corner-shop and small-format retailers that make their money from the products GLP-1s disrupt: salty snacks, chocolate bars, full-sugar drinks. They may even affect sales of alcohol, vapes, cigarettes, lottery tickets, and other impulse purchases.
And then, of course, the larger candy companies are at risk too, like Hersheys, Cadbury, and my dearly beloved Kellogs (cereal is basically a sugar-delivery mechanism).
No more Froot Loops? Maybe.
**The views, opinions, and recommendations expressed in this essay are solely my own and do not represent the views, policies, or positions of any other organization with which I am affiliated. This content is provided for informational purposes only and should not be considered medical, legal or investment advice.**
